
Dr. G. Malar, Post-Doctoral Fellow & Prof S. P. Goswami, HOD–Speech-Language Pathology
All India Institute of Speech and Hearing, Manasagangothri (University of Mysore)
Mysuru – 570 006, Karnataka, India.
Childhood is a pleasurable phase in the life of any individual where the primary occupation is growing by way of playing. Nevertheless, it is a crucial phase that has to be conducted carefully and constructively so that young children grow into self-actualised and socially-contributing adults. However several children are impeded in this process both in the form of inherent disorders or disabilities and/or deprivations and discriminations in the environment. The former was conventionally considered to be of three primary types – sensory impairments, physical-motor impairments, and cognitive impairments. More recently, there is growing awareness and acknowledgment of disorders of another nature, that is, emotional-behavioural problems. Many of these arise from or are associated with neurodevelopmental disorders.
Clinically neurodevelopmental disorders (henceforth referred to as NDD) are viewed as delays, deficiencies or deviances from typical development in children which are caused by damages or dysfunctions that occur in the central nervous system. These in turn originate from several causes of genetic, medical, environmental and/or socio-cultural nature. The causes could be triggered as early as the prenatal phase when complex neurological development commences in the foetus. They may continue to occur until after even three years of age till the process is almost complete. Subsequently, the brain functioning in growing children is affected resulting in diverse adverse consequences. Their ability to process auditory, visual and/or other sensory information received from the environment may be distorted. These distorted perceptions in turn may elicit disarrayed behaviours in response. Their psychological abilities to learn and remember can be affected. The maturation of socio-emotional skills necessary to deal adequately with the environment is also critically affected in many of these children (Dietrich, 2005; European Union, 2003; Rice & Barone, 2000).
Severe adverse outcomes of behavioural and intellectual disorders of neurodevelopmental origins may manifest in the form of disabling conditions such as attention deficit and hyperactivity disorder, autism spectrum disorders, intellectual disability and learning disabilities apart from auditory and visual processing disorders. In some regions of the world such as North America, physical-motor, as well as functional abnormalities, are also brought into the ambit of NDD. Thus it comes to encompass conditions such as cerebral palsy and other developmental disorders of coordination as well as stereotypic movements (American Psychiatric Association, 2014).
The presence of anyone or combinations of these conditions, according to nature and severity, are found to have a permeating effect on sensory processing, motor execution, cognitive perception and processing, intrapersonal adjustment, behavioural manifestations, communication and interpersonal interactions in the affected children. These complications lead to countless, complicated challenges faced by these children in the educational context. Nevertheless as of now, as Herwegen, Ashworth and Palikara (2019) report, confirmed evidence about implications of NDD in the educational domain and the prospects of special educational intervention are found to be diminished in general. They also report very many contradictions between available evidence. These scientific scarcities are attributed both to complexity and diversity in the manifestations of NDD, as well as the nascent phase in the evolution of relevant educational services. At the large presence of NDD is found to affect elementary sensory-motor, cognitive and socio-emotional functions necessary for children to survive and succeed in their educational endeavours.
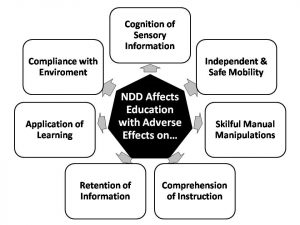
Figure 1. Educational implications of neurodevelopmental disorders.
The presence of these disabling conditions may prevent or make it difficult for children to perceive and get oriented to the environmental circumstances in the educational setting. Once inside the learning environment, some of these children find it difficult to comply with the classroom conventions and directions which are primarily conservative and conveyed verbally. Many of these children face difficulty in perceiving and processing instruction which again is verbal in nature supplemented with its secondary written and/or textual form along with optional visual representations. Their ability to visualise and comprehend verbal instruction is imperfect mostly resulting in rote learning and poor retention. Further, when they have to explain the knowledge gained or understood through spoken or written words, many children with NDD are found with deficient expressive skills. Or in higher order of learning, they may be expected to perform practical applications in new situations or for solving problems. Again in several instances, children with NDD are deprived or left with distorted skills for meaningful practical application. If problems in controlled or coordinated movements of neurological origin are also considered, then the children are faced with added difficulties in mobility and manual ability that may affect their independent functioning – both for personal and educational purposes. These constraints in functioning independently, dealing with instructional information, as well as conflicts encountered in adapting to the environment at times makes them struggle to self-regulate behaviours that are forbidden or unwelcome in the learning environment. Ultimately, children challenged with neurodevelopmental problems are more often presumed to be misfit and/or malfunctioning in terms of constructive educational efforts and outcomes (European Union, 2003; Herwegen, Ashworth, & Palikara, 2019). Even so, multifaceted rehabilitation interventions are being evolved to meet these multifarious challenges.
Clinical Rehabilitation for Neurodevelopmental Disorders
Considering the neurological origins of NDD, remedy for molecular and electrophysiological deficits through genetic or pharmacological manipulations form a pivotal role in the clinical rehabilitation of these conditions. Efforts have been directed towards investigating affected neurobiological mechanisms in case of specific disorders and attempt to modify them so as to alleviate the outcomes of these disorders (Hagerman & Hendren, 2014; Hamilton, 2015). Cognitive rehabilitation is another crucial aspect of clinical rehabilitation. Ahn and Hwang (2017; 2018) following a systematic review of research evidences published between 2006 and 2016 enumerated diverse effective cognitive therapeutic techniques ranging from behaviour therapy to occupational therapy. These are found to exert a comprehensive beneficial influence on the developmental domains of cognitive, motor, communication, social and behavioural functioning. Especially, cognitive behaviour therapies are reported to exert appreciable influence on the adaptive behaviour of the affected children. On the other hand, cognitively oriented occupational therapy has been effective in developing fine motor skills and enhancing organisation skills for executing activities of daily living as well as learning. Cognitive behaviour therapy along with occupational therapy was also found to resolve sensory issues, like hyper or hyposensitivity and/or sensory craving, which frequently hinder typical functioning in children with NDD (Lucas et al., 2016; Weston et al., 2016).
Communication and interpersonal interaction is a major casualty in almost all incidences of NDD. Hence therapies for improving communication, speech and language skills form an integral core of the clinical intervention efforts. According to the nature of the specific disabilities, the primary focus is on restoring verbal communication skills for self-sustenance by expressing basic life needs. Synchronised efforts for social-assimilation through training for sharing of thoughts and emotions with the people around are also carried out. Subsequent intervention includes the secondary form of written language in the process of educating these children and then preparing them for impending vocation. If the severity of the disorders prevents children with NDD from becoming fluent in verbal communication, it may be supplemented or substituted with other non-verbal forms of communication involving visual aids or manual forms of communication. The process requires individualised approach which is flexible to meet the particular child’s capabilities, constraints and concurrent life needs (Thapar et al., 2017).
Evolution of Educational Habilitation for Children with Neurodevelopmental Disorders
Concurrent with attempts to restore basic developmental skills through clinical intervention, efforts are undertaken to educationally habilitate children affected with NDD. The evolution of special educational services for children with diverse special needs; whether arising out of sensory, physical-motor or neurodevelopmental disorders; has followed a similar pattern. That is exclusion from educational opportunities either due to extreme-rejection or excessive-benevolence; followed by marginalisation. Marginalisation was initially relentless and rigorous in the form of segregated special schools for centuries together. Later gradual inroads were made into the mainstreams of education under the preview of integrated education since the mid-twentieth century. Nevertheless more often these children ended up being marginalised within the precincts of self-contained special classrooms or resource rooms within the general school. Ultimate endeavours to make children with special needs an integral part of general education took the form of inclusive education following the declaration of the framework of action for special education at the UNESCO-sponsored international conference convened at Salamanca in Spain in 1994 (Tremblay, 2007; UNESCO, 1994).
Educational endeavours of children with NDD followed a slightly altered course. For a long time, the import and impact of NDD were not adequately realised or recognised. Either they were mistaken for other disabilities. For example, deficits in auditory and visual processing were tagged to respective sensory impairments; so were autistic features and learning deficits to intellectual disability. Or else they were misunderstood as wanton misbehaviour. However, more recently realistic cognizance about the origins, nature and implications of these disorders are unfolding and gaining holds. Either due to progressive awareness or because of alterations in demographics and life-styles, the prevalence rates of these disorders is also surging in magnitude over the years (Center for Disease Control and Prevention, 2007; 2009; 2010).
Following increased alertness and awareness, children with NDD are exposed to a slightly different treatment in the mainstreams of education. Children with physically obvious conditions like cerebral palsy and Down’s syndrome or drastically conflicting behaviours such as hyperactivity and autism spectrum disorders are less welcome than children with less conspicuous conditions such as learning deficits or mild intellectual disability. This does not imply that their subsistence is better off. Reduced levels of recognition also implied relegated understanding of the conditions. The differential abilities of these children were poorly understood or rather misunderstood, thus leading to refused fulfilment or rebuked special educational needs. Neither neglect nor rejection of these children in the general streams of education stands well with the spirit of inclusion. Inclusive education in the real sense demands necessary accommodations and reasonably permissible modifications to satisfactorily meet the special educational needs of children with disabilities including NDD. At the same time, they are to be treated on par with their typically developing peers with optimal opportunities to interact, learn and grow along. This obligation applies to all mainstream learning environments from early childhood care and education centres, through general schools, to colleges and other higher education centres. The onus of fulfilling this mammoth obligation is to be shared by all concerned shareholders from policy-making and planning administrators, through service-delivering teaching and non-teaching staff, to service-receiving children and their caregivers as well as the larger public. To ensure such meaningful inclusion, advocates of the philosophy and practice recommend a four-pronged stratagem involving capable human resources adopting engaging instruction and equitable evaluation in the least restrictive environments (Lawrie et al., 2017; Ministerial Advisory Committee – Children & Students with Disability, 2017).
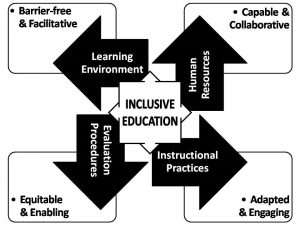
Figure 2. Constructive elements of inclusive education.
Ensuring Effectual Educational Inclusion of Children with Neurodevelopmental Disorders
Educational management of children with NDD requires coordinated action and reaction of all concerned collaborators in general education, namely, staff, caregivers, and children. The facilitative functioning has to happen at two levels. To begin with, children with NDD are to be understood, accepted and appreciated along with the differences in their adaptive behaviours and modus operandi. This in turn will help better adjustments in the learning environment, thus drawing out the best possible learning achievement. Consequently enabling optimal learning and growing both in children with and without special needs in the mainstreams of education (Irvine & Lynch, 2009).
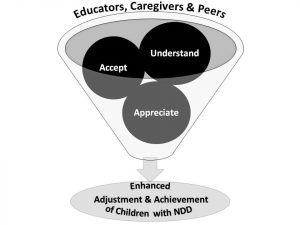
Figure 3. Factors facilitating inclusive education of children with NDD.
Catering to the special educational needs of children with NDD is a complex and challenging task compared to managing children with physical disabilities that are sensory or motor in nature. As more often than not the underlying problems are subtle but intense, mostly manifesting in outward appearances and behaviours that might be deceptive. This might be due to the interplay of psycho-social and emotional factors, thus implying the need for a careful and considerate approach in their educational management. For example, children with autistic features in the mainstream classrooms are at times observed indulging in incessant loud screaming, singing, or irrelevant repetitive utterances. It might create an impression among unacquainted educational caregivers that these children revel in loud environments, or are noise-prone by nature. In response, they may try to regulate their behaviours with voluble censures and directions. However, it is suggested that in several instances, these noisy behaviours are actually a means of expressing discomfort in raucous and riotous surroundings often encountered in large classrooms. Many children with NDD are found lacking in verbal communication and interpersonal skills to express their distress effectively. Hence, when they are disturbed with the noise in the environment, they try to mask the undesirable sounds or shut themselves out of them by reciprocating with louder sounds of their own. Therefore, raised voices or admonitions from others around will only further aggravate their disagreeable behaviours (Griffin, 2018; Sanz-Cervera et al., 2017).
The crucial issues, that make children with NDD seem odd and out-of-place in the mainstream classroom, are varied and vastly in variance among them. But the most commonly noticed problems in most of them are – indifference to beings or happenings in the environment; inability to adapt to the course of events, especially amidst changing circumstances; intolerance and extreme reactions to uncomfortable and unexpected conditions; incompetence to communicate or interact meaningfully with people around; and incapability to comprehend and comply with demands in the learning environment among others (Eldar et al., 2010; Emam & Farrell, 2009). In order to deal with such conditions effectively, while also directing efficient instruction, a three-pronged strategy shall be useful to teachers and significant others playing active or passive roles in the delivery of educational services.
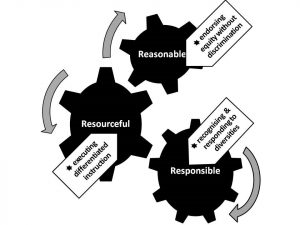
Figure 4. Dynamics of inclusive educational management of neurodevelopmental disorders.
Responsibility for Recognising and Responding to Diverse Dispositions
The foremost responsibility in managing children with NDD in the mainstream classrooms is becoming aware of their differential mode of functioning, specific special needs and the difficulties encountered in the educational context. This understanding of the condition is wasted if unaccompanied with alertness for their manifestations and keenness to resolve. As mentioned afore, the cause and effect of difficulties are distorted and not easy to identify or associate in children with NDD. Hence, their educational service providers and caregivers should consult professional rehabilitators to equip themselves with relevant practical knowledge (Burns et al., 2009).
Gaining awareness essentially involves realisation that prior prevention is better than ensuing reparations of problems. This requires cautious consideration of antecedent causes and consequent effects of the problematic issues and constant lookout for them in the learning environment. For instance, educational caregivers should be conscious that in spite of all instructional factors under their control arranged optimally, aspects beyond human manipulation such as inclement weather and consequent intolerable humidity in the classroom might put off a child with NDD leading to meltdowns. In many instances, children with NDD themselves will not be particularly conscious of the source of distress but will respond with exaggerated perceptions and extreme reactions. The intense, inappropriate reactionary behaviours of these children will distract and disturb their peers in the general classroom, disrupting habitual instructional process and discipline (Emam & Farrell, 2009; Longenecker et al., 2007).
The anticipative attitude on part of educational caregivers should keep them ever ready to manage the unanticipated with creative alternate solutions. The first step in this direction is to help both children with NDD and their peers realise and rationalise the cause of the distress. This will help bring down the acuteness of the reactions if not do away with it altogether. If in their control, they may try to remove the causative factor. If not they should try to divert the instructional course away from it with constructive compensatory action. As in the above example, indoor humidity disturbing classroom routines may be overcome with an alternate outdoor instructional activity. And at no point in time in the course of events, it will do good to blame the atypical behaviours in the children with NDD or inadequacies in the circumstances (Beckman et al., 2018; Melendez et al., 2020). Such a positive approach accentuated with acceptance will gradually ingrain constructive adjustment behaviours in children with NDD as well.
Resourceful Execution of Differentiated Instruction
Besides managing of teething troubles, another challenge confronting educational caregivers is the task of conducting instruction that benefits all children in the inclusive classroom. And at the same time ensuring individualised attention to the special educational needs of children with NDD. The widely recommended contemporary means for this from the inclusive educational perspective is the execution of a ‘Universal Design for Learning’. This implies that educational caregivers have to be prepared with the flexible, multi-strategic approach for organising instruction. This in turn will involve three-fold operations; originating with the presentation of instruction, and complemented with the engagement of the children in the process, as well as their active participatory responses (Hall et al., 2012; Rao & Meo, 2016).
Implementation of such an inclusive process will imply that children with NDD have to be rendered instruction in accessible forms and formats including appropriate language involving multisensory information. In the process, innovative means and interesting activities are to be employed for drawing and sustaining their attention in the learning tasks. Educational caregivers are also obliged to progressively inculcate self-regulatory behaviours that are conducive to inclusive instruction while discouraging distractive or disruptive trends. Ultimately, evidence for effective teaching-learning is accumulated in the form of appropriate reactions to the instructional process as well as accurate responses to the assessment measures on part of the children. In the event of such demands, children with NDD are to be encouraged to do so in viable means – verbal, visual, or practical. Necessary supports are to be extended to help them coordinate their actions and execute the activities, so as to put forward the best possible performances (Denning & Moody, 2013; Douglas & Steffen, 2016; Goodman & Williams, 2007; Hall et al., 2012). Such differentiated opportunities to receive and respond to instruction will enable all children including those with NDD to come out with optimal performances, thus leading to better achievement in given circumstances.
Reasonable Execution of Equity without Discrimination
Affirmative adjustments between children with NDD and their physical and social environment have to be receptively acknowledged. Enhanced achievement in these children following differentiated instruction has to be encouragingly appreciated. Acknowledgment and appreciation of positive outcomes of the efforts to meaningfully include children with NDD in the mainstream learning environment have to be constructive in nature. That is, every effort of theirs to chip in, not just the ones that resulted in tangible results, have to be accredited. Criticizing children for unattained targets or unfulfilled expectations may not be useful. Rather realistic feedback about possibilities for further improvement along with concrete suggestions regarding the means to realise them will be supportive (Hopfenbeck, 2020; Ovando, 1992).
In the process of doing so, it is crucial to ensure that there is no conspicuous discrimination between children with and without significant special needs. Inclusive educational caregivers have to be conscious of the fact that all children are special and unique in their own ways. Efforts to cater to this individuality at times, especially when constrained by disabilities or disorders, may involve actions of positive discrimination. These may take the form of additional benefits or concessions. In such situations, it is necessary to make sure that all concerned, including peers and their caregivers, understand the rationale behind such motives and are motivated to contribute to the process. For instance, instead of complaining about individual oral tests administered to children with NDD as an act of partiality, caregivers of their peers could be convinced to volunteer for the roles of readers and/or scribes to ensure impartiality.
As much as possible these treatments could be camouflaged in the form of collaborative learning that includes alternate options for other children as well. Definite, structured strategies have not been spelt out for such accomplishments. The means and mode have to be creatively conceived according to the context. Team project work in which children assume diverse responsibilities that are pertinent to their learning abilities and styles, but are of comparable complexity and difficulty is one widely acclaimed workable way. However, such measures are easier said than done, requiring sensitive, sensible and seasoned organisation on part of educational caregivers. All told, cooperative functioning and collective appreciation of efforts of all children in the inclusive learning environment will lead to advantageous learning and inclusive development of everyone with diverse ability, cultural, economic and social credentials (Ainscow, 2020; Choi et al., 2017; Sailor, 2016).
References
Ahn, S., & Hwang, S. (2017). Cognitive Rehabilitation with neurodevelopmental disorder: A systematic review. NeuroRehabilitation, 41(4), 707-719; doi: 10.3233/NRE-172146.
Ahn, S., & Hwang, S. (2018). Cognitive rehabilitation of adaptive behavior in children with neurodevelopmental disorders: A meta-analysis. Occupational Therapy International, 2018(5029571), n.p.; doi: 10.1155/2018/5029571.
Ainscow, M. (2020). Inclusion and equity in education: Making sense of global challenges. Prospects, 49, 123–134; doi: 10.1007/s11125-020-09506-w.
American Psychiatric Association. (2014). Diagnostic and statistical manual of mental disorders–DSM (5thed.). Arlington, VA: American Psychiatric Publishing.
Beckman, L., Janson, S., & von Kobyletzki, L. (2018). Associations between neurodevelopmental disorders and factors related to school, health, and social interaction in school children: Results from a Swedish population-based survey. Disability Health Journal, 9(4), 663-72; doi: 10.1016/j.dhjo.2016.05.002.
Burns, K. A., Leblanc, L., & Richardson, W. (2009). Autism spectrum disorder and the inclusive classroom: Effective training to enhance knowledge of ASD and evidence-based practices. Teacher Education and Special Education, 32(2), 166-179; doi: 10.177/0741932507334279.
Center for Disease Control and Prevention. (2007). Prevalence of autism spectrum disorders – Autism and Developmental Disabilities Monitoring Network, United States 2002. Morbidity and Mortality Report, 56(SS-1), pp. 12-28.
Center for Disease Control and Prevention. (2009). Prevalence of autism spectrum disorders – Autism and Developmental Disabilities Monitoring Network, United States 2002. Morbidity and Mortality Weekly Report, 58(SS10), pp. 1-20.
Center for Disease Control and Prevention. (2010). Increasing prevalence of parent-reported attention-deficit/hyperactivity disorder among children – United States 2003 and 2007. Morbidity and Mortality Weekly Report, 59(44), pp. 1439-1443.
Choi, J. H., Meisenheimer, J. M., McCart, A. B., & Sailor, W. (2017). Improving learning for all students through equity-based inclusive reform practices: Effectiveness of a fully integrated schoolwide model on student reading and math achievement. Remedial and Special Education, 38(1), 28-41; doi: 10.1177/0741932516644054.
Denning, C. B., & Moody, A. K. (2013). Supporting students with autism spectrum disorders in inclusive settings: Rethinking instruction and design. Electronic Journal for Inclusive Education, 3(1), article 6.
Dietrich, K. (2005). Principles and practices of neurodevelopmental assessment in children: Lessons learned from the centers for children’s environmental health and disease prevention research. Environmental Health Perspectives, 113(10), 1437-1446.
Douglas, K., & Steffen, S. (2016). Strategies that work for students with autism spectrum disorder in inclusive classrooms [PPT Slides]. From OAR – Organization for Autism Research. https://education.illinoisstate.edu/downloads/ntcon/Douglas1.
Eldar, E., Talmor, R., & Wolf-Zukerman, T. (2010). Successes and difficulties in the individual inclusion of children with autism spectrum disorder (ASD) in the eyes of their coordinators. International Journal of Inclusive Education, 14(1), 97-114; doi: 10.1080/13603110802504150.
Emam, M. M., & Farrell, P. (2009). Tensions experienced by teachers and their views of support for pupils with autism spectrum disorders in mainstream schools. European Journal of Special Needs Education, 24(4), 407-422; doi: 10.1080/08856250903223070.
European Union. (2003). Draft baseline report on neurodevelopmental disorders in the framework of the European environment and health strategy. Brussels, Belgium: Technical Working Group on Priority Diseases, Subgroup Neurodevelopmental.
Goodman, G., & Williams, C. M. (2007). Interventions for increasing the academic engagement of students with autism spectrum disorders in inclusive classrooms. Teaching Exceptional Children, 39(6), 53-61.
Griffin, K. (2018, December 17). Auditory sensitivity: Signs, causes and how to help. Retrieved January 25, 2021, from GriffinOT: https://www.griffinot.com/auditory-sensitivity-autism-sensory/
Hagerman, R. J., & Hendren, R. L. (2014). Treatment of neurodevelopmental disorders: Targeting neurobiological mechanisms. Oxford, UK: Oxford University Press. E-book doi: 10.1093/med/9780199937806.001.0001.
Hall, T. E., Meyer, A., & Rose, D. (Eds.). (2012). Universal Design for Learning in the classroom: Practical applications. New York, NY: Guilford Press.
Hamilton, D. R. (2015). Treatment of neurodevelopmental disorders: Targeting neurobiological mechanisms. Journal of Developmental & Behavioral Pediatrics, 36(6), 425; doi: 10.1097/DBP.0000000000000183.
Herwegen, J. V., Ashworth, M., & Palikara, O. (2019). Views of professionals about the educational needs of children with neurodevelopmental disorders. Research in Developmental Disabilities, 91(103422), n.p.; doi: 10.1016/j.ridd.2019.05.001.
Hopfenbeck, T. N. (2020). Making feedback effective? Assessment in Education: Principles, Policy and Practice. 27(1), 1-5; doi: 10.1080/0969594X.2020.1728908.
Irvine, A. N., & Lynch, S. L. (2009). Inclusive education and best practice for children with autism spectrum disorder: An integrated approach. International Journal of Inclusive Education, 13(8), 845-859; doi: 10.1080/13603110802475518.
Lawrie, G., Marquis, E., Fuller, E., Newman, T., Qui, M., Nomikoudis, M., Roelofs, F., & van Dam, L. (2017). Moving towards inclusive learning and teaching: A synthesis of recent literature. Teaching & Learning Inquiry, 5(1), n.p.; doi: 10.20343/teachlearninqu.5.1.3.
Longenecker, H., Mace, C., Perry, L., & Steege, M.W. (2007). Applied behavior analysis: Beyond discrete trial teaching. Wiley Periodicals, Incorporated, 44(1), 91-99; doi: 10.1002/pits.20208.
Lucas, B. R., Elliott, E. J., & Coggan, S. (2016). Interventions to improve gross motor performance in children with neurodevelopmental disorders: A meta-analysis. BMC Pediatrics, 16(1), 193.
Melendez, A. B., Malmsten, M., Einberg, E.-L., Clausson, E. K., & Garmy, P. (2020). Supporting students with neurodevelopment disorders in school health care — School nurses’ experiences. International Journal of Environmental Research and Public Health, 17(5752), n.p.; doi: 10.3390/ijerph17165752.
Ministerial Advisory Committee – Children & Students with Disability. (2017). Principles of inclusion for children and students with disability in education and care. Adelaide, Australia: Government of South Australia.
Ovando, M. N. (1992). Constructive feedback: A key to successful teaching and learning. Austin, TX: Department of Educational Administration, College of Education, the University of Texas at Austin.
Rao, K., & Meo, G. (2016). Using ‘Universal Design for Learning’ to design standards-based lessons. SAGE Open, 2016(October-December), 1-12; doi: 10.1177/2158244016680688.
Reagan, N. (2012, April). Effective inclusion of students with autism spectrum disorders. M. S. Special Education thesis submitted to Ralph C. Wilson, Jr. School of Education. Rochester, NY: Fisher Digital Publications, St. John Fisher College.
Rice, D., & Barone, J. S. (2000). Critical periods of vulnerability for the developing nervous system. Environmental Health Perspectives, 108(S3), 511-533.
Sailor, W. (2016). Equity as a basis for inclusive educational systems change. Australasian Journal of Special Education, 12, 1-17; doi: 10.1017/jse.2016.12.
Sanz-Cervera, P., Pastor-Cerezuela, G., González-Sala, F., Tárraga-Mínguez, R., & Fernández-Andrés, M.-I. (2017, October 11). Sensory processing in children with autism spectrum disorder and/or attention deficit hyperactivity disorder in the home and classroom contexts. Frontiers in Psychology, 8(1772), n.p.; doi: 10.3389/fpsyg.2017.01772.
Thapar, A., Cooper, M., & Rutter, M. (2017). Neurodevelopmental disorders. Lancet Psychiatry, 4(4), 339-346; doi: 10.1016/S2215-0366(16)30376-5.
Tremblay, P. (2007). Special needs education basis: Historical and conceptual approach [PPT Slides]. From Université Libre de Bruxelles – http://www.ibe.unesco.org/sites/default/files/History_Inclusive_Education.
United Nations Education, Scientific and Cultural Organisation–UNESCO. (1994). The Salamanca Statement and Framework for Action on Special Needs Education. Salamanca, Spain: UNESCO.
Weston, L., Hodgekins, J., & Langdon, P. E. (2016). Effectiveness of cognitive behavioural therapy with people who have autistic spectrum disorders: A systematic review and meta-analysis. Clinical Psychology Review, 49, 41-54.




