Dyslexia identification is a process that incorporates multiple sources of information and includes screening, assessment, intervention or instruction, and progress monitoring

Screening in dyslexia supports early identification and intervention for those at risk. The information provided here is intended to help establish and support screening initiatives by clarifying the terminology and approaches.
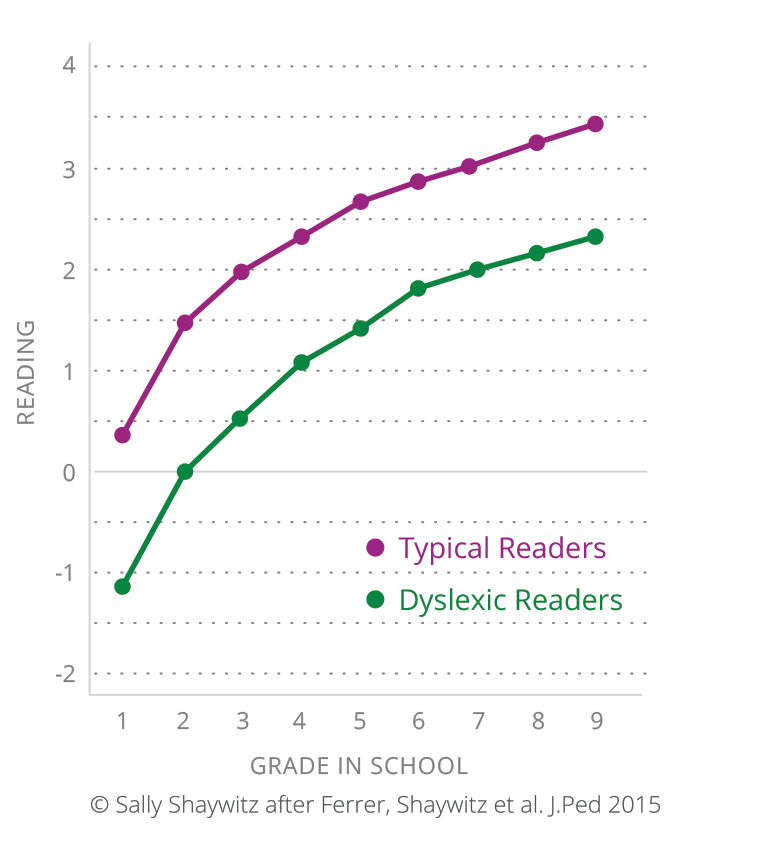
The achievement gap between typical and dyslexic readers is already present, impacts students as early as first grade, and persists over time. Early screening combined with high-quality, evidence-based interventions are essential for closing this achievement gap.  The incidence of Dyslexia in India is believed to be 15% which brings the count to about 35 million dyslexic Indian children. (Source: Dyslexia Association of India)
The incidence of Dyslexia in India is believed to be 15% which brings the count to about 35 million dyslexic Indian children. (Source: Dyslexia Association of India)
Screeners are brief measures that are intended to sort individuals into two groups—those at risk and those not at risk. Some screeners use a cut score-that is, a “cut-off’ score—that divides the two groups
 There are two broad categories of screeners:
There are two broad categories of screeners:
(1) Performance-based measures, which require the person being screened to complete specific tasks
(2) Rating scales, which require a rater, such as a teacher or parent, or the individual being screened to respond to a series of statements or questions by providing each one with a rating.
Screeners are evaluated based on the following characteristics:
Use of the screener is supported by sound scientific evidence, including strong reliability and validity data. Sufficient information about the measure is reported to allow for critical evaluation and replication.
The screener’s reliability coefficients provide evidence that the items are internally consistent. Studies may also be conducted to determine whether the results are stable over time and across scorers/raters.
The screener measures what it claims to measure. For example, it may show strong correlations with other established measures in the field. The most important type of validity evidence for a dyslexia screener is clinical validity, evidence that the screener will accurately classify children at risk for dyslexia by significantly differentiating between individuals with and without dyslexia.
The clinical validity of a screener is evaluated based on the following characteristics:
Sensitivity: The strength of a screening measure in finding true positives-that is, individuals who have dyslexia.
Specificity: The strength of a screening measure in eliminating true negatives—that is, individuals who do not have dyslexia.
AUC (Area under the Receiver Operating Characteristics curve): AUC estimates range from .50 (chance accuracy) to 1.00 (perfect accuracy). Many of the strongest performing clinical assessment inventories deliver AUC estimates in the 0.7 to 0.8 range. 
Universal screening is a general education effort that:
Universal dyslexia screening is a first step within an overall dyslexia identification process.
 Effective universal screening balances the accuracyand power of the measure (e.g., reliability and validity, clinical sensitivity, and specificity) with the practical issues related to the application of the screener in a school environment. These issues can include the time needed to administer, student time away from instruction, and cost.
Effective universal screening balances the accuracyand power of the measure (e.g., reliability and validity, clinical sensitivity, and specificity) with the practical issues related to the application of the screener in a school environment. These issues can include the time needed to administer, student time away from instruction, and cost.

 Age Range: Grade K-1Learn More
Age Range: Grade K-1Learn More Age Range: 4:6 to 6:5Learn More
Age Range: 4:6 to 6:5Learn More Age Range: 6:6 to 11:5Learn More
Age Range: 6:6 to 11:5Learn More Age Range: 11:6 to 16:5Learn More
Age Range: 11:6 to 16:5Learn More Age Range: 16:5 to ∞Learn More
Age Range: 16:5 to ∞Learn More




